Autoimmune hemolytic anemia
Download as PPTX, PDF19 likes9,811 views

This document discusses autoimmune hemolytic anemia (AIHA). It begins by defining hemolytic anemia and classifying it as either congenital/hereditary or acquired. It then discusses the classification of hemolytic anemias as either intracorpuscular or extracorpuscular. The mechanisms, clinical features, laboratory findings, and treatments of warm AIHA and cold AIHA are described in detail. Warm AIHA is mediated by IgG antibodies and most commonly involves the Rh blood group antigen. Cold AIHA involves IgM antibodies reactive below 37°C and usually targets the I antigen. Corticosteroids are first-line treatment for warm AIHA while cold AIHA may be associated with underlying infections or malignancies.


![CLASSIFICATION OF HEMOLYTIC ANEMIAS
INTRACORPUSCULAR EXTRACORPUSCULAR
DEFECTS FACTORS
HEREDITARY •HEMOGLOBINOPATHIES
•ENZYMOPATHIES
•MEMBRANE-
CYTOSKELETAL DEFECTS
•FAMILIAL HEMOLYTIC
UREMIC SYNDROME
ACQUIRED •PAROXYSMAL •MECHANICAL DESTRUCTION
NOCTURNAL [MICROANGIOPATHIC]
HEMOGLOBINURIA •TOXIC AGENTS
•DRUGS
•INFECTIOUS
•AUTOIMMUNE](https://image.slidesharecdn.com/autoimmunehemolyticanemia-200731144155/85/Autoimmune-hemolytic-anemia-3-320.jpg)




![GENERAL FEATURES
OF HEMOLYTIC DISORDERS
GENERAL EXAMINATION - JAUNDICE, PALLOR
BOSSING OF SKULL
PHYSICAL FINDINGS
HEMOGLOBIN
MCV
RETICULOCYTES
BILIRUBIN
LDH
HAPTOGLOBULIN
- ENLARGED SPLEEN
- FROM NORMAL TO SEVERELY REDUCED
- USUALLY INCREASED
- INCREASED
- INCREASED[MOSTLY UNCONJUGATED]
- INCREASED
- REDUCED TO ABSENT](https://image.slidesharecdn.com/autoimmunehemolyticanemia-200731144155/85/Autoimmune-hemolytic-anemia-8-320.jpg)















































































Autoimmune hemolytic anemia
- 1. AUTO IMMUNE HEMOLYTIC ANEMIA CHAIR PERSON:DR SACHIN HOSKATTI STUDENT: AKSHATHA K
- 2. HEMOLYTIC ANEMIA Definition: Those anemias which result from an increase in RBC destruction coupled with increased erythropoiesis Classification: Congenital / Hereditary Acquired
- 3. CLASSIFICATION OF HEMOLYTIC ANEMIAS INTRACORPUSCULAR EXTRACORPUSCULAR DEFECTS FACTORS HEREDITARY •HEMOGLOBINOPATHIES •ENZYMOPATHIES •MEMBRANE- CYTOSKELETAL DEFECTS •FAMILIAL HEMOLYTIC UREMIC SYNDROME ACQUIRED •PAROXYSMAL •MECHANICAL DESTRUCTION NOCTURNAL [MICROANGIOPATHIC] HEMOGLOBINURIA •TOXIC AGENTS •DRUGS •INFECTIOUS •AUTOIMMUNE
- 4. CLASSIFICATION Intravascular hemolysis MAHA Transfusion rx PNH Infections Snake bite Extravascular hemolysis Hemoglobinopathies Enzymopathies Membrane defects AIHA
- 7. HOW TO DIAGNOSE HEMOLYTIC ANEMIA New onset pallor or anemia Jaundice Splenomegaly Gall stones Dark colored urine Leg ulcers
- 8. GENERAL FEATURES OF HEMOLYTIC DISORDERS GENERAL EXAMINATION - JAUNDICE, PALLOR BOSSING OF SKULL PHYSICAL FINDINGS HEMOGLOBIN MCV RETICULOCYTES BILIRUBIN LDH HAPTOGLOBULIN - ENLARGED SPLEEN - FROM NORMAL TO SEVERELY REDUCED - USUALLY INCREASED - INCREASED - INCREASED[MOSTLY UNCONJUGATED] - INCREASED - REDUCED TO ABSENT
- 10. HEMOLYTIC FACIES- CHIPMUNK FACIES
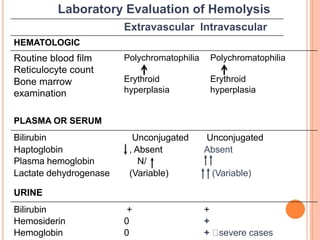
- 11. Laboratory Evaluation of Hemolysis Extravascular Intravascular HEMATOLOGIC Routine blood film Reticulocyte count Bone marrow examination PLASMA OR SERUM Polychromatophilia Erythroid hyperplasia Polychromatophilia Erythroid hyperplasia Bilirubin Unconjugated Unconjugated Haptoglobin , Absent Absent Plasma hemoglobin N/ Lactate dehydrogenase (Variable) (Variable) URINE Bilirubin + + Hemosiderin 0 + Hemoglobin 0 + severe cases
- 12. CASE SCENARIO 1 A young male patient who is a soldier presented with complaints of passage of dark urine immediately following physical exertion in the upright position, occasionally accompanied by nausea, abdominal cramps, aching in the back or legs, a “stitch in the side,” or a burning feeling in the soles of the feet . Physical examination is transient jaundice usually unrevealing, hepatosplenomegaly and transient jaundice have been rarely reported
- 13. Post exercise, his urine sample was reddish brown in color with a specific gravity of 1.030, pH 5.5, 1+ protein, 3+ blood, 0 to 2 RBC/high powered field (HPF) and 0 to 2 white blood cells/HPF. His urine microscopy revealed 1 to 2 RBC/ HPF.
- 15. IMMUNE HEMOLYTIC ANEMIA: When erythrocytes are destroyed prematurely by an immune mediated process (antibody and/or complement), the disorder is referred to as an immune hemolytic anemia(IHA). Autoimmune hemolytic anemia Drug-induced hemolytic anemia Alloimmune hemolytic anemia
- 16. AUTOIMMUNE DRUG INDUCED ALLOIMMUNE Warm-reactive antibodies Primary or idiopathic Secondary 1. Autoimmune disorders (SLE,RA, and others) 2. Chronic lymphocytic leukemia and other immunoproliferative diseases 3. Viral infections 4. Neoplastic disorders 5. Chronic inflammatory diseases Cold-reactive antibodies Primary or idiopathic (cold hemagglutinin disease) Secondary 1. Infectious diseases (mycoplasma pneumoniae, EBVand other organisms) 2. Lymphoproliferative disorders 3. Paroxysmal cold hemoglobinuria Mixed - type Drug adsorption Immune complex Autoantibody induction Membrane modification Hemolytic transfusion reaction Hemolytic disease of the fetus and newborn
- 17. CLINCAL SCENARIO 2 Zohra begum,40yrs,female Chief complaints: yellowing of skin,fatigue since 5 months,ulcer at back since 3 months On examination:pallor+,icterus + P/A examination splenomegaly + Other systemic examination normal I/V: Retic count :3.6% LDH:1062U/L DIRECT COOMB’S + ANA +
- 19. AUTOIMMUNE HEMOLYTIC ANEMIA AIHA is a complex and incompletely understood process characterized by an immune reaction against self-antigens and shortened erythrocyte survival . Individuals produce antibodies against their own erythrocyte antigens (autoantibodies). The autoantibodies characteristically react not only with the erythrocytes of the individual but also with the erythrocytes of other individuals carrying the antigen.
- 21. SITES AND FACTORS THAT AFFECT HEMOLYSIS Hemolysis can be intravascular or extravascular Erythrocytes sensitized with antibody or complement components attach to macrophages in the spleen or liver via macrophage receptors for the Fc portion of immunoglobulin or the C3b component of complement. These cells are then phagocytized . Intravascular hemolysis occurs if the complement cascade is activated through C9 (the membrane attack complex). INTRAVASCULAREXTRAVASCULAR
- 25. MECHANISM OF HEMOLYSIS IgG- Mediated Hemolysis Complement Mediated Hemolysis IgM-Meddiated Hemolysis
- 27. IgG mediates erythrocyte destruction by first attaching to the erythrocyte membrane antigens through the Fab portion of the Ig molecule. Fc receptors on macrophages in the red pulp of the spleen bind to the Fc portion of the attached IgG After binding, the macrophage pits the antigen antibody (Ag/Ab) complex, fragmenting the cell membrane spherocyte RIGID LESS DEFORMABALE Phagocytosed by splenic macrophages
- 31. IGM MEDIATED HEMOLYSIS Macrophages doesn’t have receptors for Fc portion IgM IgM is efficient activator of complement EXTRAVASCULAR: - complement activation incomlete - C3b coats RBCs and sensitised cells destroyed extravascularly via CR1 and CR3 receptors on macrophages IgM can agglutinate cells in addition to activating complement.
- 32. LABORATORY IDENTIFICATION OF SENSITIZED RED CELLS When immune hemolytic anemia is suspected, tests to detect and identify the causative antibody are indicated. In general, two distinct techniques are used: • Agglutination in saline, which will detect antibodies of the IgM class • Antihuman globulin (AHG) test, which will detect antibodies of the IgG class and/or complement
- 33. ANTIHUMAN GLOBULIN TEST: IgM antibodies can be detected by agglutination reactions between test sera and appropriate erythrocytes suspended in saline. Erythrocytes Zeta potiential(25nm) Direct: detects erythrocytes coated with antibody in vivo Indirect: detects antibodies in the plasma or serum
- 38. WARM AUTOIMMUNE HEMOLYTIC ANEMIA Most common form of AIHA (70% of cases) Incidence-1/50,000 -75,000 Mediated by IgG antibodies whose maximal reactivity is at 37°C. • Primary or idiopathic: no underlying disease • Secondary: underlying disease present • Lymphoproliferative disease • Neoplastic diseases • Autoimmune disoders • Viral and bacterial infections • Vaccinations
- 39. Diseases or Conditions Associated with Warm Autoimmune Antibodies Autoimmune disorders Systemic lupus erythematosus Rheumatoid arthritis Scleroderma Ulcerative colitis Antiphospholipid antibodies Lymphoproliferative disorders Chronic lymphocytic leukemia Acute myelocytic leukemia Hodgkin lymphoma Non-Hodgkin lymphoma Waldenström macroglobulinemia Other lymphoproliferative disorders Multiple myeloma
- 40. Other neoplastic disorders Thymoma Ovarian dermoid cyst Teratoma Kaposi sarcoma Carcinoma Viral infections Epstein-Barr virus Hepatitis C virus HIV/AIDS Other Diphtheria-pertussis-tetanus vaccinations Pregnancy Bone marrow transplantation Congenital immune deficiency states Hypogammaglobulinemia Dysglobulinemia
- 41. ANTIBODY CHARACTERISTICS Immunochemistry and Origin Most antibodies are IgG (IgG1>IgG3) Blood Group Specificity Warm autoantibodies are panagglutinins Rh is the most common (70%), Other blood group include Wright (Wrb), Ena, Duffy (Fyb), Gerbich (Ge), Kidd (Jka), Kell (K), Lutheran (Lu), LW, M, N, S, Pr, A, B, IT, Sc3, U, Vel, and Xga .
- 42. PATHOPHYSIOLOGY The warm autoantibody in AIHA is reactive with antigens on the patient’s erythrocytes. Specificity of the antibody is directed against antigens of the Rh system. Most hemolysis in WAIHA is extravascular via splenic macrophages. If both antibody and complement are on the cell membrane, phagocytosis is enhanced. Direct complement- mediated intravascular hemolysis associated with IgM antibodies in warm AIHA is rare.
- 44. CLINICAL FEATURES: Idiopathic AIHA: Progressive weakness, Dizziness, Dyspnea on exertion, Back or abdominal pain, Jaundice. Secondary AIHA: patient can present with signs and symptoms of both the underlying disease and hemolysis or just the disease.
- 47. Laboratory Findings Associated with WAIHA Common findings Other laboratory findings that can be associated with hemolysis in WAIHA Positive DAT Normocytic, normochromic anemia Increased reticulocytes Spherocytes and other erythrocyte abnormalities Presence of autoantibody in the serum Increased serum bilirubin (total and unconjugated) Decreased serum haptoglobin Positive antibody screen with all cells including autocontrol Incompatible crossmatches with all donors Increased osmotic fragility Increased urine and fecal urobilinogen Hemoglobinemia,* hemoglobinuria, methemoglobinemia, hemosiderinurea
- 49. THERAPY: CORTICOSTEROIDS: Glucocorticoids are the initial therapy of choice for warm AIHA Dose:1.0 to 1.5 mg/kg or 40 mg/m2/day of prednisone or its equivalent. Response: noticeable by 7 days. Tapering: Rapid responders can reduce their dose by 50% over 4 to 6 weeks, tapering should proceed more slowly over 3 to 4 months
- 50. SPLENECTOMY Splenectomy is indicated in those surgical candidates who have not responded to prednisone, And who requires prednisone doses >10-20 mg/day to maintain remission, or Intolerable side effects.
- 51. IMMUNOSUPPRESSIVE THERAPY Immunosuppressive regimen might include • 80 mg/m2/day • or AZATHIOPRINE • 60 mg/m2/day • or CYCLOPHOSP HAMIDE • 40 mg/m2/day PREDNISONE
- 52. Rituximab: is a chimeric human/murine monoclonal anti-CD20 antibody Mycophenolate mofetil: Doses begin at 1 g/day and are then increased to 2 g/day. Cyclosporine A: Doses of 3 mg/kg/day with target serum levels of 200–400 ng/ml • 375 mg/m2/week × 4 weeksRituximab
- 53. Other Therapies Intravenous immunoglobulin (IVIG) has not enjoyed the success in AIHA that it has in immune thrombocytopenia. Escalating the dose from the standard 0.4 g/kg/day (× 5 days) to 1.0 g/kg/day may be helpful. Plasmapheresis
- 54. COLD AUTOIMMUNE HEMOLYTIC ANEMIA (AIHA) Cold AIHA, also termed cold agglutinin disease (CAD), is associated with an IgM antibody that fixes complement and is reactive below 37°C. This disorder, which comprises 16–30% of the AIHAs IgA and IgG antibodies rarely have been implicated in hemolysis in CAD
- 55. ANTIBODY CHARACTERISTICS Immunochemistry and Origin: Cold agglutinins are IgM. Specificity for the I antigen: I antigen-90% i antigen-10% Adult RBCs are used to detect anti-I agglutinins and cord RBCs are needed to detect anti-i agglutinins. M. pneumoniae induces anti-I antibodies in the majority of patients is potentially related to the finding that sialylated I/i antigens serve as specific Mycoplasma receptors
- 56. Secondary Cold Agglutinin Disease Neoplasms Waldenstrom macroglobulinemia Angioimmunoblastic lymphoma Other lymphomas Chronic lymphocytic leukemia Kaposi sarcoma Myeloma Nonhematologic malignancy (rare) Infections Mycoplasma pneumoniae Mononucleosis (Epstein-Barr virus) Adenovirus Cytomegalovirus Encephalitis Influenza viruses Rubella
- 57. Rubella Varicella Human immunodeficiency virus Mumps Ornithosis Legionnaires disease Escherichia coli Subacute bacterial endocarditis Listeriosis Syphilis Trypanosomiasis Malaria Other Autoimmune diseases Tropical eosinophilia
- 59. PATHOPHYSIOLOGY: The severity of CAD is related to the thermal range of the antibody(up to 32%) I antigen specificity Cold-reacting antibody is usually directed against the I antigen. The second most common specificity for cold autogglutinins is anti-Pr.1.
- 62. CLINICAL FEATURES Mild, chronic hemolytic anemia with exacerbations in the winter. and jaundice may occur if the rate of hemolysis is greater than the endogenous capability to metabolize bilirubin . Intermittent bursts of hemolysis associated with hemoglobinemia and hemoglobinuria on exposure to cold. Acrocyanosis can occur from agglutination of RBCs in the cooler vessels of the hands, ears, nose, and feet. Digits may become cold, stiff, painful, or numb and may turn purplish Chronic CAD patients have mild splenomegaly or hepatomegaly
- 67. THERAPY The most effective therapy is usually achieved by keeping the individual’s extremities warm. Chemotherapy using cyclophosphamide or chlorambucil can be instituted(Underlying lymphoproliferative disease) Plasma exchange. Rituximab has been used as treatment in both primary and secondary disease. Chlorambucil, beginning with 2 to 4 mg/day and increasing by 2 mg every 2 months Pulse therapy with cyclophosphamide (250 mg/day) and prednisone (100 mg/day × 4 days) every 2 to 3 weeks
- 68. CASE SCENARIO 3 A four-year-old male presents to the emergency department with a history of six days of fever and acute onset of red colored urine. There has been no recent travel. He was seen by his Doctor approximately five days ago for evaluation of cough and rhinorrhea and was prescribed Antibiotics for an ear infection.No h/o dysuria, bloody stools, hemoptysis, or epistaxis. He has no increased bruising, no petechiae, and no extremity pain. He has been having intermittent fevers for three days. Physical Exam: (+) scleral icterus, (+) jaundice, (+) soft flow murmur on cardiac exam. Physical exam is otherwise normal.
- 69. LABS: Initial hemoglobin 10.4 g/dL--> decreased to 6.3 g/dL 12 hours later, Platelets 153,000 cells/UL, Reticulocyte count 0.4%, White blood cells 11.1 x103cells Coagulation studies normal. Liver function test are normal. LDH is 5056 Units/ml, Haptoglobin 12 mg/dL (low). Unconjugated bilirubin is 3.7 mg/dL, Conjugated bilirubin is 1.2 mg/dL. Electrolytes are all within normal limits. Viral panel is pending. DAT: IgG, C3 (+). Urinalysis: dark, red-brown urine, 3+ blood, 3+ protein, 0-4 RBCs/hpf, 0-4 WBCs/hpf, urobilinogen >8mg/dL.
- 70. PAROXYSMAL COLD HEMOGLOBINURIA Characterized by massive intermittent acute hemolysis and hemoglobinuria. Can occur at any age ,frequently seen in children less than 5 years. The infections linked to PCH include Epstein-Barr virus, Cytomegalovirus, Measles, mumps, Heamophilus influenzae, Klebsiella pneumoniae. Parvovirus 19, Onset : 5 days to 3 weeks after onset of the infection
- 71. PATHOPHYSIOLOGY Donath-Landsteiner (D-L) antibody. Biphasic refers to the two temperatures necessary for optimal lysis of the erythrocytes. The antibody reacts with erythrocytes in the capillaries at temperatures less than 20°C and avidly binds the early acting complement components. The antibody molecule disperses from the cell, but the membrane attack complement components are activated on the cell membrane causing cell lysis. TEMP <20°C TEMP @37°C
- 72. CLINICAL FINDINGS Hemoglobinuria Jaundice Pallor Hepatosplenomegaly Raynaud’s phenomenon
- 73. LAB INVESTIGATIONS Neutropenia. Reticulocytopenia. Serum bilirubin, BUN, and LD are elevated Serum complement and haptoglobin are decreased. DAT with anticomplement antisera :Weakly positive. IAT can be positive if performed in the cold D-L antibodies :low titres(1:32)
- 76. THERAPY PCH associated with acute infections terminates upon recovery from the infection. Steroids are not usually helpful. Transfusion can be required if the hemolysis is severe. In rare cases when the hemolysis persists, plasmapheresis can be used. Rituximab (anti-CD20) has also been used as therapy
- 77. MIXED-TYPE AIHA Mixed-type AIHA is characterized by the presence of a warmreacting IgG autoantibody and a cold- reacting IgM autoantibody that has both high titer and increased thermal amplitude. About 50% of the cases are idiopathic. Associated with diseases such as systemic lupus erythematosus, lymphoma, and HIV. Patients usually respond well to treatment with corticosteroids and do not require transfusion. Rituiximab has been used in cases with underlying lymphoproliferative disease
- 78. DRUG-INDUCED HEMOLYTIC ANEMIAS It is recognized that certain drugs can cause immune cytopenias that involve one or several cell lines including neutrophils, platelets, and erythrocytes. Three classic hypotheses • Drug absorption • Immune complex formation • Autoantibody induction
- 85. CASE SCENARIO 32 yr old presented 4 days history of distention of abdomen and rt hypochondrial pain and has h/o passage of dark colored urine at night for weeks On USG- hepatomegaly,gross ascites,hepatic vein thrombosis Lab : Hb – 7gm%. WBC- 2200, PLC- 80,000 LDH- 600, S.BR- 4 mg% urine bile pigment +,heme dip stick++ What is the diagnosis
- 86. CASE SCENARIO 14 YR old female present with anemia, jaundice Rt hypochondrial pain o/e-vitals stable.pallor+,icterus+,splenomegaly + Usg- cholilithiasis Lab; elevated ,LDH, S.Bilirubin Peripheral smear shows
- 87. CASE SCENARIO 25 yr old male with RHD – severe MR done MVR,after 10 days presented with pallor, palpitation,jaundice CBC shows Hb – 7.5 gm %, Hct -22 % Lab : S.bilirubin -4.5mg% LDH -600 Retic count 10% Peripheral smear –
- 88. REFERENCES: Wintrobe’s Clinical Hematology 12th Edition Williams Hematology 9E Harrison’s principles of Internal Medicine Pearson New International Edition Clinical Laboratory Hematology Shirlyn B. McKenzie Second Edition
- 89. THANK YOU